CEMENTED AND CEMENTLESS TOTAL HIP REPLACEMENTS
| |||||||||
| CONTENTS:
cementless total hip prosthesis some special techniques prostheses for revision operations Purpose of the fixation of the prosthesis to the skeleton The total hip prosthesis must be anchored securely within the skeleton for good function. The loose sitting total hip prosthesis is painful and such loose total hip is also stiff. There are two methods how to secure the fixation of a total hip prosthesis to the skeleton:
The construction, the form, and the rehabilitation after the operation with these two types of prostheses are different. 1The cemented total hip prosthesisThe cup and the shaft of a cemented total hip prosthesis are fixed to the skeleton with a self curing polymer compound called bone cement. The bone cement fills completely the space between the skeleton and the surface of the prosthesis. But bone cement is not a true glue, it is only filling material.
Benefits and disadvantages of the cemented prostheses The advantages The cemented total hip replacement tolerates small deviations from the precise operation technique. The bed cut for the prosthesis in the skeleton need not to be very exact because the bone cement filler will level out all incongruities. The patients can put weight on their new total hips immediately after the operation (in theory). Actually, the strength of the fixation of the cemented total hip to the skeleton is most strong at the end of the operation. The factor that limits full weight bearing is the surgical damage to the soft tissues around the total hip. These tissues must heal before the full weight bearing is possible. The cement layer also acts as an intermediate bumper between the very stiff metal of the total hip prosthesis and the weak skeleton. This bumper levels the peak forces acting on the skeleton around the total hip during gait. The disadvantages are two: One is that pressing the doughy bone cement into the raw bone marrow cavity during the operation may cause circulatory disturbances. The other is that the bone cement ages, cracks, and after some time the bond between the prosthesis and the skeleton may be lost. 2The cementless total hip prosthesis
The components of the total hip prosthesis are pushed (press-fitted or blown into) directly in the space made by the surgeon in the skeleton and held there by the elastic forced generated in the bone tissue. The form of the total hip prosthesis must be adapted for the cementless fixation. First, the polyethylene or ceramic cups of the cementless prostheses must be enshrouded within a metallic encasing before they are pushed into the reamed space in the acetabulum. Bone tissue does not stand direct contact with polyethylene or ceramic materials of the cup and polyethylene or ceramic cup in direct contact with raw bone would loosen. These cementless cups are thus relatively thick; their wall consists of the polyethylene or ceramic inner cup ("lining") plus the metallic encasing. In the metal-on-metal total hip devices the metallic cup is pushed into place directly and needs not any encasing. It follows that the wall is is relatively thin (about 5-6 millimeters). Second, the surface of the shaft component must be made rough. A smooth surface of the shaft component will slide against the walls of the marrow cavity and will not adhere directly to the skeleton of the thigh bone. A smooth shaft component of a cementless total hip will not achieve stable fixation in the skeleton A rough surface of the shaft component will improve the immediate fixation of the shaft component to the skeleton. As yet, the most effective rough surface is the porous coating applied on the surface of a cementless total hip.
Benefits and Disadvantages of cementless THR Advantages of cementless total hip replacement: The surgeon avoids all problems with cementing the total hip during the operation (problems with mixing the bone cement, waiting for hardening of the doughy bone cement, changes of the position of prosthetic components while the bone cement is still in doughy state, risk of blood pressure fall and heart failure during cementing of the prosthesis) The patient avoids the risk that the bone cement layer will crack and successively disintegrate years after the operation. Disadvantages of cementless total hip replacement There is a risk that chunks of the bone marrow substance will be pushed into the circulation during the forceful hammering of the cementless total hip into place. The need for restricted weight bearing 6-12 weeks (not always) Pain in the thigh, sometimes > 1 year Risk of a fracture of the skeleton during operation, when the surgeon blows the total hip too vigorously into an undersized bony bed. Loosening of the metallic balls or fibers from the porous coated surface. These balls may land inside the total joint between the bearing joint surfaces and act as a third body. These hard metallic surfaces then accelerate the wear from these surfaces. Spongy metal
The trabecular metal has one big advantage: its mechanical characteristics come very close to the mechanical characteristics of the spongious bone itself. It is thus used mainly in reconstructive procedures where it replaces the lost bone. So the bioengineers often use trabecular metal to make parts of skeleton, for example parts of a destructed pelvis bone, from this material. Whereas the traditional porous coatings allows ingrowth of bone tissue some tenths of a milimeter, the trabecular metal allows much greater ingrowth of bone tissue. _______________________________________ The weight bearing after cementless THR If the surgeon succeeded to impact firmly the cementless total hip prosthesis onto the raw bone surfaces, the prosthesis will not move during walking, thus the bone tissue growing into the porous surface of the prosthesis will not be damaged by the early weight bearing. If the prosthesis was not impacted firmly onto the raw bone surfaces, every time the patient makes a non-protected step the porous surface of the prosthesis moves against the skeleton and cuts the newly formed sprouts of bone tissue. Eventually, only loose fibrous tissue will connect the unstable cementless prosthesis to the skeleton. Such loose attachment may cause pain and failure of the cementless total hip prosthesis. Thus, the surgeons usually recommend non weight bearing regime for 6 -12 weeks after a cementless total hip prosthesis to enhance the biologic fixation of the prosthesis. Simultaneous bilateral TH and weight bearing The ban of the immediate postoperative weight bearing may be a problem for patients with cementless bilateral total hip replacements. Several surgeons allow, however, their patients with bilateral cementless total hips " weight bearing as tolerated" on two crutches or on a walker immediately after the operation, if the cementless total hip prostheses were stable after the impacting. The immediate weight bearing in these patients did not cause any complications, on the contrary the speed of recovery was quickened. Studies demonstrated that in patients where the surgeon succeeded to achieve a stable fixation of the cementless total hip prosthesis to the patient's skeleton, the immediate weight bearing "as tolerated" on two crutches or on a walker did not cause any harm. Some studies even maintain that the recovery of muscle force and walking capability was quicker in these patients than in patients with a non weight-bearing regime. Thus, your surgeon knows how stable the fixation of your new cementless hip is. Discuss always the question of weight bearing on your new total hip always with him.
5Cementless cup
The bone tissue cannot stand direct contact with the surfaces of polyethylene or ceramic cups. Such direct contact provokes osteolysis - bone dissolving disease. So that when the surgeon wishes to use ceramic or polyethylene cups without a protecting layer of bone cement, these cups must be put into a thin metallic casing - a metallic back-up. The cementless cup thus consists of an outer metallic layer and an inner layer made of polyethylene or ceramic, also called the liner. The liner articulates with the ball. The surface of the metallic back-up is often porous coated and has openings for screws. The surgeon impacts (blows, hammers) the metallic casing directly into the carefully prepared bony bed in the hip socket ( the acetabulum). Another name for such cup is "press-fit cup". To enhance the fixation of the metal-backed cup to the skeleton, the surgeon may put screws through the holes in the metallic casing and into the pelvic skeleton. There are also cups that may be screwed into place. The metallic back-up of these prostheses has screw wings on the outside. The cup is screwed as one large screw into reamed screw wing tracks prepared in the walls of the socket. Sandwich systems for cementless cups The relatively soft cement layer in the cemented ceramic or metallic cups provides, in theory, a bumper protection of the metallic or ceramic cups against the shocks occurring through walking and other activities. To protect the cementless metallic or ceramic total hip cups from these chocks, some manufacturers place (sandwich) a layer of polyethylene between the inner ceramic or metallic liner and the outer metallic casing. Advantages of metal-backed cups: simple operation technique Disadvantages: the liner may dislocate from the metal-backing. The liner may rotate against the metal-backing and produce additional polyethylene wear particles
6Cementless shaft:Two general features characterize the shafts of the modern cementless total hip prosthesis:
Porous coating offers immediate stability and late biological fixation of the THP
Click on the icon for a full size picture Porous coated hip stem The surfaces of the modern cementless total hip prosthesis which are in contact with skeleton are porous coated. A thin layer of very small sintered titanium balls or a very fine mesh of titanium wires is applied as porous coating on the surface of cementless total hips stems. (DePuy -Porocoat total hip)
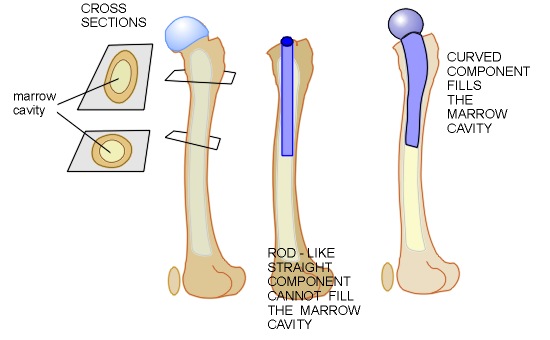
The Fit and Fill principle It is not difficult to prepare place for the spherical cup in the hip socket by reaming, but it is impossible to ream the marrow cavity so that the shaft of the total hip prosthesis would fill the marrow cavity completely and be jammed firmly in it. This is so because the marrow cavity of the thigh bone changes its shape. In the upper part it has a shape of an ellipse on cross section, whereas it has the shape of a long, S shaped rigid tube on cross-section beneath. Yet, the form of the shaft of a total hip prosthesis must accommodate to this form of marrow cavity to withstand the stresses put on the shaft by everyday life.
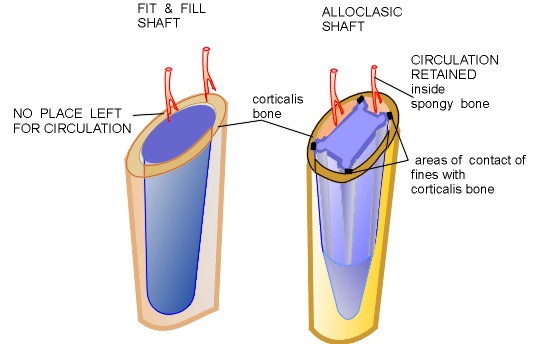
Picture: The fit and fill principle of the shaft component. (Click on the icon for a full size picture) Profile view of the thigh bone. The marrow cavity inside the shaft of the thigh bone is oblong in the upper part of the thigh bone, but it is circular in the middle part. Note also that the shaft has a S- like form. (Left side picture) Ideally the shaft of the prosthesis should be in close contact with all walls of the marrow cavity. This is impossible with a straight rod-like shaft (Middle picture) With a proprietary fluted form of the shaft the contact will be better. Such form is, however, difficult to fabricate and even more, difficult to introduce and place in the marrow cavity.(Right side picture) The bioengineers are now satisfied when the shaft of the prosthesis has contact with the inner walls of the marrow cavity at least at three places. This suffices theoretically to achieve initial stability of the shaft. The form of the commercially used prosthetic shafts is thus a compromise. The shaft is elliptic on cross section in its upper part , and it is circular and rod-like in the lower part where the marrow cavity is tube-like. It sways in some model to accommodate to the S shape of the thighbone. There are two theoretical problems associated with "fit and fill" principle.First, the femoral shaft component that fills entirely the bone marrow cavity shields the skeleton from the stresses created by the body weight. Without these stresses the skeleton around the femoral shaft becomes weak and may break through if the stress shielding is excessive. To obviate this complication, the modern cementless prostheses are in close contact with the skeleton in the upper (proximal ) part of the thighbone skeleton only. The skeleton distally (beneath) from this place is not in direct contact with the stem component and remains strong. Second, the stem component must be anchored securely in the bone marrow cavity. The contents of bone marrow cavity are loose fat tissues, blood vessels nearing the inner side of the skeleton, and weak spongy bone. The strong skeleton is on the outside, so called corticalis bone. The corticalis bone forms strong hollow tube around the bone marrow cavity. For stabile anchor, the stem component must be in contact with the strong corticalis bone. The surgeon who prepares place for a round conforming shaft component reams the bone marrow cavity and removes spongy bone together with blood vessels. The corticalis bone will thus be deprived of its circulation. Consequently accomplished, the "fit and fill" procedure thus leaves the inner half of the corticalis bloodless, dead. There are surgeons who do not accept this kind of fit and fill procedure. The Austrian surgeon Karl Zweymuller developed the Alloclassic cementless total hip. The shaft component of the Alloclassic total hip is rectangular on cross section. The contact with the corticalis bone is through four small fins. Doctor Zweymuller maintains that this cross section makes it possible to retain circulation in the bone marrow cavity in cementless Alloclassic total hip. At the same time, the rectangular and not circular shape of the femoral component gives an extra rotational stability to this prosthesis.
Picture: Fit and fill versus Alloclassic femoral component Click on the icon for full size picture. Left side: Conventional cementless stem inside the marrow cavity. The stem fills the marrow cavity completely. There is no place for vessels inside the bone marrow cavity, all space is occupied by the "fit and fill" shaft component. Note also that round shaft component placed inside the round marrow cavity is not stable against rotational forces. Right side: Alloclassic total hip. The contact of the quadrilateral shaft component with the corticalis bone is through four fines. There is space left for blood vessels between the fines. Note also that the fines that are placed in precisely reamed spaces add extra stability to the stem against rotational forces. The surgeon must, however, use special reaming instruments and ream carefully through the bone marrow cavity lest he / she do not damages the circulation inside the marrow cavity. The Allosclassic total hip is used mainly in Europe with great success. After ten years, 92% of all Alloclassic total hips survive and are working fine. (Gruebl 2002) ____________ Gruebl A et al. J Bone Joint Surg-Am 2002; 84-A:425 - 31
Stresses on the shaft of a total hip prosthesisIn the patient's body, the shaft of the total hip prosthesis must withstand two kinds of stresses The bending stress tries to bend the shaft of the prosthesis, e.g. during ordinary standing and walking. A shaft well embedded in the marrow cavity will resist well these stresses, either cemented or non cemented.
3 The porous coating What is it? The porous coating is a thin layer of a fine wire mesh or a layer of small balls sintered together, that is applied on the outer surface of the total joint prosthesis. The coating materials are pure Titanium and Cobalt -Chromium alloys, both are well tolerated by the bone tissue.
Click on the icon for a full size picture The purpose of porous coating is to enhance the fixation of the shaft to the skeleton. The sintered ball or titanium mesh makes a complicated maze. Within the wire mesh or between the individual balls there is a labyrinth of fine tunnels that attract the ingrowth of bone tissue. How thick is the porous coating layer The surface coating layer is only a few millimeters thick, fast sintered to the surface of the prosthesis component. Only tunnels of certain dimensions in the porous coating attract ingrowth of the bone tissue. The bone tissue cannot grow into openings that are very small (say < 40 thousands of a millimeter) and it will grow very slowly into openings that are too wide (say >500 thousands of a millimeter). The precise dimension of openings in the porous coating varies with the manufacturer of the porous coated prosthesis. Ingrowth of bone tissue The bone tissue will grow into the porous coated surfaces only when the porous coated surface of the prosthesis is steadily impacted against the surface of the skeleton. The closer the surface of the total hip component to the skeleton, the quicker will the bone tissue find its way into the porous surface. Bone tissue would not cross gaps between the porous surface and the skeleton that are more than 1,5 millimeters wide. It really comes to blow the cementless prosthesis in its bed! When there is a movement between the porous coated surface of the prosthesis and the surface of the skeleton the newly ingrown bone tissue, which is stiff, is cut away from its vascular sources by these movements. In the end, in a cementless total hip which moves against the skeleton, there develops only loose soft fibrous tissue between the porous coated surface and the skeleton. A prosthesis attached to the skeleton with a loose fibrous tissue is not stable.
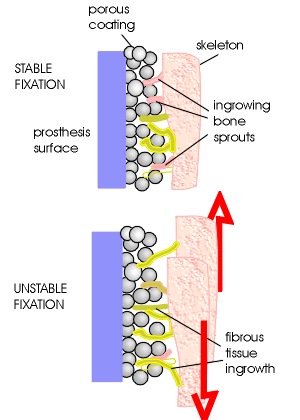
Picture: Ingrowth of tissues into the stable and unstable cementless total hip Click on the icon for a full size picture Upper picture shows a stable cementless fixation. From the skeleton close to the prosthesis grow thin sprouts of new bone tissue into the pores of the porous surface. Note that only a smaller part of the pores is occupied by the newly growing bone tissue. Observations revealed that on the average only about 30% of the porous coated surfaces are ingrown with bone. Note that there is also fibrous tissue (non bone tissue) between the prosthesis and the skeleton. In stable cementless total hips, presence of fibrous tissue on these places is beneficial. Such fibrous tissue enhances the fixation of the prosthesis an prevents access of small wear particles to the bone. Bone does not grow into the depth of the porous coating, so porous coating layer may be thin. The ingrowing sprouts of bone tissue are not strong initially, yet they will tolerate very small movements ("micromovements") between the prosthetic surface and the skeleton. With "small" the surgeons mean movements not greater than the openings in the porous coating (tenths of millimeters). Lower picture shows an unstable cementless fixation. Movements between an unstable cementless total hip prosthesis and the skeleton occur are on a larger scale (millimeters). Only the long strands of loose fibrous tissue endure these movements. No stiff bone sprouts can endure such large relative movement. Note also that the bone tissue is rosy in the picture - the bone tissue in the vicinity of the prosthesis is rarefied, more spongy-like. This state is called osteoporosis. Scientists believe that the stiff metallic components protect the neighboring bone from "natural" stresses. Non-stimulated bone tissue rarefies, becomes osteoporotic. Studies demonstrate that the skeleton around the cementless total hip had lost about 30 % of its bone content. This bone loss is not restored. Creating a stable, biological fixation With time, bone tissue grows into this sponge-like surface of a stable prosthesis and the total hip joint becomes an integrated part of the skeleton. This is called biological fixation. But even a well biologically fixed total hip still has on average only 30% of its surface ingrown with bone tissue. Animal experiments demonstrated that the strength of fixation of the cementless prosthesis to the skeleton increases successively during the first 12 postoperative weeks. After that period the strength of the fixation does not change much. That may be the reason why the patients are kept on non weight-bearing regime after the operation with a cementless prosthesis for 6 to 12 weeks. The surgeons will prohibit early loading of the total hip prosthesis that may cause undue movements between the prosthesis and the skeleton until the fixation is sufficiently strong. Surgeons usually distinguish three phases of bone ingrowth and fixation into the cementless total hip prosthesis 1) An "acute phase" lasting about 3 months. During this phase, the bone tissue damaged at the operation is removed and replaced, and the bone tissue then grows into the porous surface. 2) An adaptive phase lasting from about 3 months to 2 years postoperatively. The new bone is remodeling and reshaping incessantly. In general the skeleton around the total hip is losing about 30% of the bone tissue. On X-ray, this is seen as osteoporosis around the cementless total hip. The bone loss is mainly dependent on the mechanical characteristics of the femoral stem component. In some distinct areas of the skeleton, however, the shaft component of the prosthesis exercises more pressure on the skeleton. Skeleton reacts with formation of more bone tissues in these areas. On X-ray pictures, these areas are more white and the surgeons call these areas "sclerosis". 3) A stable phase from 2 years onward. During this phase the bone tissue is remodeling at a slower pace, responding to the stresses put on it by the cementless total hip. The volume of bone tissue does not increase in the osteoporotic areas. The changes on the X-ray pictures are small.
Hydroxyapatite coating Hydroxyappatite (HA) is a mineral that makes bone hard and strong. A synthetic variant of this mineral (which is ceramic) is available and may be put as a thin layer on the surface of the metallic porous coating. Several studies demonstrated that a thin layer of hydroxyapatite ceramic enhances the ingrowth of the bone tissue into the porous coating furthermore. The HA coated cementless total hips become stable earlier, and the bone ingrowth proceeds on a larger area ( usually about 10% larger) of the coated surface.
Some special techniquesRobotic surgery: Usually, the surgeon prepares the cavity for the prosthetic shaft in the thigh bone with drills, saws, and templates that look like instruments carpenters use Although these instruments are high precision tools, some surgeons try to improve the precision of the cutting and drilling procedures. These surgeons have been experimenting with a computer aided milling machine. This machine drills a hole through the marrow cavity after data put into the computer by the surgeon. The milling operation makes only a small part (about 10%) of the total hip operation. Yet, with the use of the Computer aided milling machine, this is is an elaborate procedure that needs extensive preparations with placing of special target wires in the thigh and taking several X-rays, all done at a separate operation one or more days before the total hip replacement operation proper. Advantages: marginally better shape of the space for the prosthetic shaft. (This is still discussed) Disadvantages: Expensive and time consuming procedure, still largely experimental not in general use. More complications. Custom made implants Some shafts are so deformed by previous disease that even a modular femoral component will not fit. For these patients, the surgeon may order a custom made femoral shaft. The patient is CT scanned ( a special X-ray technique depicting three dimensionally the form of the femoral shaft) and the pictures are sent to the manufacturer. At the manufacturers workshop, computer-assisted lathe turns a prosthetic shaft that will fit the marrow cavity of the the deformed femoral bone. This procedure takes between 1 to more weeks. The operation with such custom made femoral component proceeds as usually. Some surgeons try to improve the fit of femoral shaft also in patients without deformed femoral shafts. They manufacture the prosthetic shaft after a casting taken during the operation. The surgeon first prepares the marrow cavity of the thigh bone for the shaft of the prosthesis. He/she then makes a casting from this cavity that is sent to the technician who works close to the operation room. While the patient is asleep, the technician manufactures the customized shaft after the casting, sterilizes it and sends the ready implant to the surgeon who places the customized shaft in place and continues the operation. This procedure takes between 45 to 60 minutes, even longer in some cases. Advantages: perhaps better fit of the shaft - this is still discussed Disadvantages: Expensive and time consuming procedure, still experimental. The quality of the shaft is dependent on the characteristics of the metal suitable for quick turning the shaft. Cobalt chrome alloys cannot be used for this purpose. The mechanic characteristic can be inferior due to lack of the mechanical control of the quickly manufactured component More complications due to long anesthesia time, more bleeding, higher risk of postoperative infection. Using current surgical techniques, most patients can be fitted with the standard cementless modular shafts. Prostheses for revision operationsThe osteolysis destructs the skeleton around a total hip prosthesis. The round socket in the acetabulum (pelvic bone) after the primary operation is changed into a large irregular cavity, sometimes communicating with the abdominal cavity. The fine S shaped form of the marrow cavity in the thigh bone is lost and replaced with a large cavity with very thin walls.
The surgeon who should replace the loose prosthesis with a new implant, faces a difficult problem how to fill these cavities. For this purpose the manufacturers produce special revision total hip prostheses that are bulkier than ordinary hip prostheses. The revision cups are extra large and have several screw holes for a firm attachment to the healthy part of the pelvic skeleton. The shafts of the revision prostheses are extra long. Their lower part should be anchored in the lower part of the thigh bone which has still healthy marrow cavity. The shafts are often available as a "box of bricks" with different sizes of components. This is called modular construction.
Figure: "Box of bricks" shafts. Click on the icon for a full size picture. The surgeon assembles the right size of the prosthetic shaft from these "bricks" directly at the operation table. For very large destruction even the modular stem will not fill the defect in the skeleton. The surgeon has then a choice to order a custom-made prosthesis directly from the manufacturer. The manufacturer produces the custom made shaft according to special (CT) X-ray pictures. There is still discussion ongoing whether the revision total hip prosthesis should be cemented or cementless. For more information visit please also the following chapters Loosening of total hip joints
Before you take any action, please read carefully the DISCLAIMER
|